Whenever I would encounter something, I would write on a scrap piece of paper thinking that it would be good to review and make post out of.
However, this practice was lost in between my procrastination and laziness.
Today as I witnessed tarsorrhaphy (sewing eye lids shut) for the first time, and then I realized I must write about this. After all, my time at the clinic was ending and perhaps this would serve as a good reminder when I have to study ophthalmology.
The patient was a frail woman, octogenarian.
The procedure done was very similar to this, except both medial and lateral corners were done so that there was a 'tiny peep hole' in case something happened to her good eye.
The reason why the mucous membrane is shaved is because cells adhere better.
Sort of like debridement in a way, it just heals better.
The healing was especially important part as the woman had shingles and therefore had lost all her sensation.
"No sensation, No healing"
The reason why tarsorrhaphy is done can be divided to 4 main reasons:
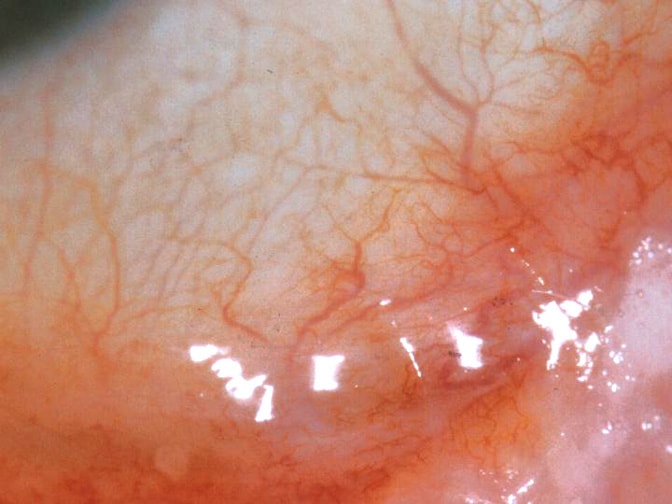
1. Neuroparalytic :Neuroparalytic keratitis is inflammation of the cornea as a sequel to interruption of sensory impulses over the fifth (trigeminal) cranial nerve. The cornea’s loss of sensitivity leaves it much more subject to injury, exposure, and infection.
2. Neurotrophic
3. Corneal disease
4. Decrease exposure.
HERPES ZOSTER --> SHINGLES --> CN 7/ CN 5 damage --> ECTROPION/KERATITIS --> ECTROPION REPAIR/ worst case: TARSORRHAPHY
and as you might have guessed, the woman suffered from shingles and suffered terrible keratitis.
HM (Hand Movement) and LP (Light Perception) was the only vision she had left.
She hardly felt anything was the local anesthetic was given to her (usually "for 7 seconds it hurts like hell!" but "hurts going in but not coming out").
Indeed the surgery was done accordingly and smoothly.
I hope her quick recovery.
*
When CO2 laser is used it can blow 'air' in and can result in subcutaneous emphysema (I google it and it says sometimes referred to Sub Q Air).
Emphysema means 'trapped air'
Usually this can also happen if someone gets DCR (dacrocystorhinostomy) because some bone is removed and so when a person blows his/her nose really hard, it can happen.
*
It is always so difficult to leave the 'position' because you become familiar with it and you identify yourself with the position.
I've had in total about 4 different position here and each leave was 1) Silent (Mutual?) 2)Lots of Yelling P/O 3) Voluntary half fired half? 4) Voluntary
I was given exit review.
1. What did you enjoy the most while working here?
Learning. To be able to witness and participate in all aspect of patient care including reception to screening and assisting was an amazing experience! The sense of fulfillment and really feeling like a part of a team working efficiently together for excellent patient care was another part I enjoyed thoroughly.
2. What did you find the most frustrating?
I don't think I was ever frustrated with anything.
3. Did you feel that management supported you?
Definitely, I was grateful for management's understanding with my volunteer and family commitment.
4. Were you given appropriate training?
Yes, while the course from SAIT provided me with academic guidance on-the-job training and guidance provided by all the other staffs (Olga, Teresa, Cheryl, Angela and Mary) helped me enormously and gave me practical understanding.
5. Were you fairly treated? were your accomplishments acknowledged?
I believe so. Yes, staffs were very appreciative and I was always so flattered.
6. Was your salary reasonable and appropriate
It was discussed.
7. Were your working condition satisfactory?
Sometimes long hours were exhausting (10 hours) but I have no complaints because I enjoyed the OR time
8. What are our office's strengths?
Strong team work, staffs' dedication to excellent patient care, professionalism, efficient staffs, caring environment, friendliness to mention few.
9. What are our office's Weaknesses?
Can't think of any
10. What would you like to see change at the office?
I would not change much, because I considered the office the most ideal in terms of how the clinic should be run. However, I wish sometimes people could be more courteous to one another if they are having a bad day because it is really infectious.
11. Are there any other areas you'd like to discuss?
Thank you very much for everything. I feel so lucky to have worked at this office and feels sorry for leaving, because I can't imagine a better office environment to work.