Antithesis to myself.
I look at others in such way.
Expecting their hard-earned path,
only gained through months and years of suffering.
Then I see people who do it so effortlessly.
10 years, short or long.
It is what it is.
Difference in age then is,
mere 2 years.
In those 2 year differences, I see so many things built.
Another degree.
Marriage.
And on way to tenure ship.
Have you ever seen anything else so smooth?
Amazing, amazing I said,
couldn't be helped so amazed.
The odds, the chances, the probability! I wondered
Perhaps to thee, my exclamation might be bemused statement,
but I say to thee, I'm simply amazed.
The odds I ask,
The interviews I ask,
I want to ask more questions, but I don't want to be viewed impolite.
Although I might have made myself seem rude.
I wonder about path so smooth.
Something that are meant to be.
Perhaps they were meant to be.
Can I change my path?
Do I dare?
Tuesday, 19 February 2013
Thursday, 14 February 2013
Feb 14: Lessons with Dr.J ; April: asking questions
How do you react to patients with difficult prognosis?
Thyroid eye disease is a terrible thing.
So far I have learned that:
Hypothyroid : treats with either synthroid, dessicated thyroid, levothyroxine
Hyperthyroid: treats with tapazole or beta-blockers (especially those who are allergic to tapazole).
Never mind all that primary or secondary disorder because I don't remember.
I know that Hyperthyroid --> heat, eat more but wasted, sweaty and tired all the time --> thin
Hypothyroid --> usually overweight (doesn't eat much but easily gain weight)
Treated with either thyroidectomy or radioactive iodine, thyroid eye disease may develop in either.
To be specific, thyroid eye disease is different from the actual thyroid disorder (Grave's (hyper), or Hashimoto's, or hypo or hyper) as ALL can develop thyroid eye disease. Reasons as explained in another post: Here
A patient walks in with stylish sunglasses and begin to tell me about the episode she had last Saturday and that Dr. J already knew about this, as the resident made phone call to Dr.J at 7am in the morning on Sat.
She has never felt any intense pain in her eyes before.
She has used drugs that costs thousands and had injections twice.
Yet, when the problem should be stagnant, it keeps on developing and evolving into grimmer situation.
There's no answer.
She might tears.
What do I do? is what she asks
What should professionals do in this case?
I could feel tears coming up - putting myself into her shoes.
Having to live with that.
Doing everything and no real progress. Not even a stop to its development.
Radiation treatment 1/3 of what is used to treat cancer, he says. But later, he adds, after we try this.
Giving prescription to the lady, asking her to not to get into argument with her loved ones and sell or buy any big things like house, property or cars (side effect of prednisone)
We will get through this.
We need to stop that.
That's what he says.
We have to be the calm one, then I realized.
We have to be the professionals.
Update made in April 2013
Dexamethasone (swelling) vs. Prednisone (inflammation) in use for thyroid eye disease.
If dexamethasone is 6.6 times more potent than prednisone (when you calculate the dose required for every 10mg of dexamethasone, approx 66mg of prednisone is needed). I then wondered why use prednisone when you have rampant thyroid eye disease, wouldn't it be better to use low dose dexamethasone.
I asked Dr. J this one day and he was honest with me that he couldn't remember exactly but that dexamethasone is glucocorticoid and so is prednisone but mineralcorticoid action in prednisone is very minor. He also mentioned from the end of his memory that the efficacy, and potency differences as well.
I tried to find if there are any comprehensive guidelines that firmly says why prednisone might be better but I haven't found a good source yet.
Thyroid eye disease is a terrible thing.
So far I have learned that:
Hypothyroid : treats with either synthroid, dessicated thyroid, levothyroxine
Hyperthyroid: treats with tapazole or beta-blockers (especially those who are allergic to tapazole).
Never mind all that primary or secondary disorder because I don't remember.
I know that Hyperthyroid --> heat, eat more but wasted, sweaty and tired all the time --> thin
Hypothyroid --> usually overweight (doesn't eat much but easily gain weight)
Treated with either thyroidectomy or radioactive iodine, thyroid eye disease may develop in either.
To be specific, thyroid eye disease is different from the actual thyroid disorder (Grave's (hyper), or Hashimoto's, or hypo or hyper) as ALL can develop thyroid eye disease. Reasons as explained in another post: Here
A patient walks in with stylish sunglasses and begin to tell me about the episode she had last Saturday and that Dr. J already knew about this, as the resident made phone call to Dr.J at 7am in the morning on Sat.
She has never felt any intense pain in her eyes before.
She has used drugs that costs thousands and had injections twice.
Yet, when the problem should be stagnant, it keeps on developing and evolving into grimmer situation.
There's no answer.
She might tears.
What do I do? is what she asks
What should professionals do in this case?
I could feel tears coming up - putting myself into her shoes.
Having to live with that.
Doing everything and no real progress. Not even a stop to its development.
Radiation treatment 1/3 of what is used to treat cancer, he says. But later, he adds, after we try this.
Giving prescription to the lady, asking her to not to get into argument with her loved ones and sell or buy any big things like house, property or cars (side effect of prednisone)
We will get through this.
We need to stop that.
That's what he says.
We have to be the calm one, then I realized.
We have to be the professionals.
Update made in April 2013
Dexamethasone (swelling) vs. Prednisone (inflammation) in use for thyroid eye disease.
If dexamethasone is 6.6 times more potent than prednisone (when you calculate the dose required for every 10mg of dexamethasone, approx 66mg of prednisone is needed). I then wondered why use prednisone when you have rampant thyroid eye disease, wouldn't it be better to use low dose dexamethasone.
I asked Dr. J this one day and he was honest with me that he couldn't remember exactly but that dexamethasone is glucocorticoid and so is prednisone but mineralcorticoid action in prednisone is very minor. He also mentioned from the end of his memory that the efficacy, and potency differences as well.
I tried to find if there are any comprehensive guidelines that firmly says why prednisone might be better but I haven't found a good source yet.
Wednesday, 30 January 2013
Jan 30 - Lessons with Dr. J
Hyperventilation and Emesis (Vomiting):
"Remember the case this Monday?", says Dr.J
"yes" I squeaked.
Last Monday, I appeared to be apprehensive in Dr. J's eyes, when I expressed my worries that patient had told me that she had a extreme case of a needle phobia.
ap·pre·hen·sive
/ˌapriˈhensiv/
Adjective
| |
Synonyms
|
so back to today.
We had an unusually long surgery in one case... because of the 'red stuff'.
Later when I failed to have the patient follow my breathing instruction, Dr. J told me, "you have to coach" I observed as the Nurse waited for her to take her instruction.
"Remember we are professionals, so we have to take 'control' of the situation and lead the patient - do you know any parents controlled by their children? - it's a disaster. - we have to be the one reassuring patients."
said Dr.Johnson - as T came over and calmed the patient down and she went back to normal breathing --> less bleeding --> quicker surgery.
As patient was hyperventilating, he asked me a question.
"What happens when patient hyperventilate?".
And as always I fumbled...
[just like I did when we discussed the reason why Dr. J put pilocarpine in one eye that he was operating on:
"I couldn't find any reason based on her chart....aniscoriasis?".
"...you mean aniscoria?" -
Reason: Asian & hyperopia (aka farsightedness) - concluded from + A/R reading ("that's why A/R reading is important!) --> conclusion: smaller eye (shallow anterior chamber and narrow angle)--> leading to higher risk for Angle closure (Closed angle) glaucoma because a) smaller eye ...
"and bright light? so dilation...?"
"that causes constriction!"
"Right, SNS!!!"
"think local!"
"um (thinking alcane)...does it have Ach?" looks up at me
"no..."
"right! Epi!!" b) Epi in local anesthetic which will activate SNS and dilate pupils in addition to activation in a stressful situation --> Big pupils pushes down which means even more narrow angle - thus drop of pilo for prevention.]
"metabolic... no reproductive..not respiratory acidosis?"
"you have CO2 out, so that's alkalosis"
"I remember it being counter intuitive because of the bicarbonate (HCO3).... "
So moving on to next surgery, I couldn't let go and said,
"CO2 is going down so H2CO3 is converted to HCO3 + H+ so acidity goes up?"
and now I see that I was completely wrong!!!! how embarrassing!!!
Hyperventilation --> CO2 level decrease in blood (hypocapnia) - CO2 is carried as bicarbonate (CO2 = HCO3) (!!!!!!!) in the blood, so the loss of CO2 drives HCO3 + H+ --> Carbonic acid (H2CO3) --> H20 + CO2!! resulting loss of H+ makes blood alkaline and thus causes Metabolic Alkalosis
CO2 (g) + H20 (l) <=> H2CO3 (aq) <=> H+ (aq) + HCO3- (aq)CO2 goes down, H+ goes down fyi: it's moving <--
in other words...

it means:

fyi:
Respiratory acidosis is a condition that occurs when the lungs cannot remove all of the carbon dioxide the body produces. This causes body fluids, especially the blood, to become too acidic.
Metabolic acidosis is a condition in which there is too much acid in the body fluids.
- Diabetic acidosis (also called diabetic ketoacidosis and DKA) develops when substances known as ketone bodies, which are acidic, build up during uncontrolled type 1 diabetes
- Hyperchloremic acidosis results from excessive loss of sodium bicarbonate from the body, as can happen with severe diarrhea
- Lactic acidosis is a buildup of lactic acid. It can be caused by:
- Alcohol
- Cancer
- Exercising for a very long time
- Liver failure
- Low blood sugar (hypoglycemia)
- Medications such as salicylates
- Prolonged lack of oxygen from shock, heart failure, or severe anemia
Other causes of metabolic acidosis include:
- Kidney disease (distal tubular acidosis and proximal renal tubular acidosis)
- Poisoning by aspirin, ethylene glycol (found in antifreeze), or methanol
- Severe dehydration
Clinical implication of hyperventilation:
- lowers Intra Cranial Pressure
- Hyperventilation --> CO2 decreases --> Alkalosis --> Normally, alkalosis lowers neuronal excitability (pH: 7.4 → 7.8). Alkalosis causes H+ to move out from the cells and K+ to move in to the cell, leading to hypokalemia. This leads to a higher concentration gradient between intracellular and extracellular K+ leading to more K+ exiting the cell through leakage channels leading to hyperpolarization of the cell. This means that a greater than normal stimulus is required to reach the threshold and thus elicit a subsequent action potential.
- A major effect of alkalosis is hyperexcitability of the nervous system. Peripheral nerves are affected first, resulting in spontaneous nervous stimulation of muscles. Spasms and tetanic contractions and possibly extreme nervousness or convulsions result. Severe alkalosis can cause death as a result of tetany of the respiratory muscles
- Muscle contraction: hypocapnia causes muscular tension, poor posture, aggression and violence.
synthesis of glutamine:
“Studies designed to determine the effects produced by hyperventilation on nerve and muscle have been consistent in their finding on increased irritability” (Brown, 1953). Muscles and nerve cells become abnormally sensitive or irritated.
"Cortical CO2 tension and neuronal excitability". It was shown that CO2 has a strong calming effect on excessive excitability of brain areas responsible for thinking (Krnjevic et al, 1965).
hyperventilation "leads to spontaneous and asynchronous firing of cortical neurons"(Huttunen et. al, 1999).
= pain and bleeding?????
*
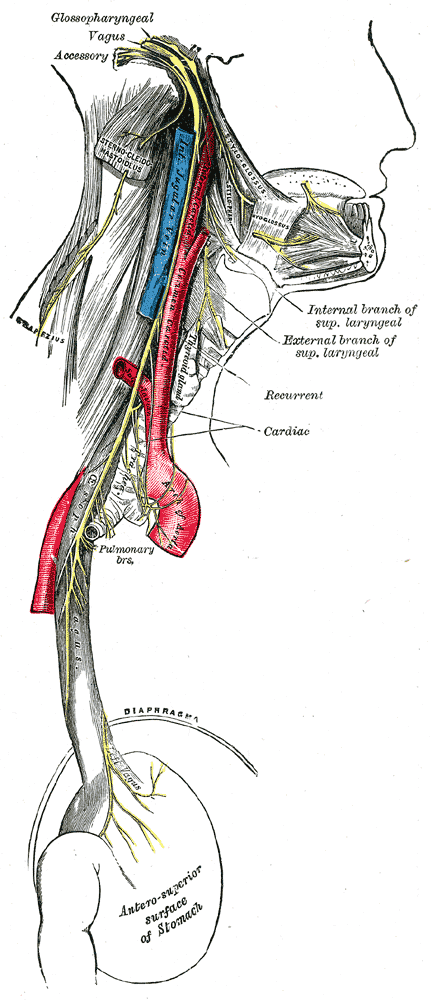
In other cases, there was emesis during surgery involving thyroid patient. (See Thyroid here!)
How can mere eye surgery cause emesis? Vagus nerve activation.
- Color of vomit
- Bright red in the vomit suggests bleeding from the esophagus
- Dark red vomit with liver-like clots suggests profuse bleeding in the stomach, such as from a perforated ulcer
- Coffee ground-like vomit suggests less severe bleeding in the stomach, because the gastric acid has had time to change the composition of the blood
- Yellow vomit suggests bile. This indicates that the pyloric valve is open and bile is flowing into the stomach from the duodenum. (This is more common in older people.)
Pressing upon certain places on the throat, sinuses, and eyes (also known as vagal reflex stimulation when performed clinically)
*
And I just remembered something about CABG (coronary artery bypass graft)...
heart bypass or bypass surgery is a surgical procedure performed to relieve angina and reduce the risk of death from coronary artery disease. Arteries or veins from elsewhere in the patient's body are grafted to the coronary arteries to bypass atheroscleroticnarrowings and improve the bloodsupply to the coronary circulationsupplying the myocardium (heart muscle). This surgery is usually performed with the heart stopped, necessitating the usage ofcardiopulmonary bypass; techniques are available to perform CABG on a beating heart, so-called "off-pump" surgery.


The terms single bypass, double bypass, triple bypass, quadruple bypass and quintuple bypass refer to the number of coronary arteries bypassed in the procedure. In other words, a double bypass means two coronary arteries are bypassed (e.g. the left anterior descending (LAD) coronary artery andright coronary artery (RCA)); a triple bypass means three vessels are bypassed (e.g. LAD, RCA, left circumflex artery (LCX)); a quadruple bypass means four vessels are bypassed (e.g. LAD, RCA, LCX, first diagonal artery of the LAD) while quintuple means five. Bypass of more than four coronary arteries is uncommon.
A greater number of bypasses does not imply a person is "more sick", nor does a lesser number imply a person is "healthier."[17] A person with a large amount of coronary artery disease (CAD) may receive fewer bypass grafts owing to the lack of suitable "target" vessels.
Saturday, 26 January 2013
Jan 21 Lessons with Dr. J and Lumps and Bumps!
This morning, as any Monday morning, I proceeded with getting the patient in, taking pictures, giving brief instruction and la~la~
Let's talk about bumps and lumps. I've been meaning to cover this base for a long, long time!
1. Chalazion - Caused by blockage of a duct that drains meibomean gland -- NON-INFECTIOUS
Treatment: apply warm compresses for 10-15 minutes qid --> soften the hardened oils blocking the duct and promote drainage and healing
Prognosis: disappear without a treatment in a month or so; if it continues to get bigger - surgically remove oil gunk - another effect: big chalazion put pressures on cornea causing astigmatism

2. If infected --> Hordeolum or Stye (external hordeola). (THINK PIMPLE! PAINFUL!)
Meibomian gland/glad of Zeis or Moll + usually bacterial (staphylococcal) infection



3. Nevus ("birthmark" L - brown, freckle like spot): sharply circumscribed and chronic lesion of the skin. This flat, benign and pigmented area may appear inside the eye or on its surface. Commonly appear on the choroid (the layer behind retina, the iris, and the conjunctiva)


4. Conjunctival Papilloma: categorized into infectious (viral), squamous cell, limbal and inverted based on appearance, location, patient's age, propensity to recur after excision, and histopathology. They are also classified based on gross clinical appearance: pedunculated (infectious conjunctival papilloma and squamous cell papilloma) or sessile.
 |
| (Sonorandeserteye) |
5. AHC (Apocrine hidrocystoma) - also cystadenoma, moll's gland cyst, sudoriferous cyst:
Hidrocystoma is cysts of the sweat glands usually on the eye lids. It is NOT tumour (hidroadenoma is)
"Whether these represent retention of cysts or benign neoplasm is controversial. When these lesions become more complex with papillary structures and increased cellularity --> cystadenoma" (DermAtlas)
 |
| Shiny skin coloured compressible cyst (DermAtlas) |
6. Syringoma: harmless sweat duct tumours clustered on eyelids (also found in armpits, ubmilicus, or vulva). They are skin-coloured or yellowish firm rounded bumps.
 |
| Syryngioma (eccrine) |












Thursday, 24 January 2013
Jan : Informed consent - Lesson with Dr. J
*
"Ok, here's one"
As he sutures patient's entropion left lower eye lid, Dr.J asks me a question what the informed consent is.
My mind boggles down to typical pre-med answers.
Informed consent to be given to patients who are mentally capable to understand the kind of procedure they are agreeing to, if not decision makers, who, looking after the patients best interest, makes a decision for the patient.
He paused for a moment and says, "informed consent is letting patients know about "risks" and "benefits" about the "intervention" vs. "non-intervention" where the communication is an absolute key. As you can't explain risks and benefits in Latin to English-only speaking patients - communication between patients and health-care providers is most important.
Informed consent from Wikipedia:
Informed consent is a phrase often used in LAW to indicate that the consent a person gives meets certain minimum standards. As a literal matter, in the absence of fraud, it is redundant.
*
Relating to informed consent.
"Patient-Centered-Care".
"Patient-focused-care, there shouldn't even be a word, for it. It sounds like Doctors are ignorant of patients if such things are to be taught."
"It's just like a chicken nugget advertising ' now with 100% chicken!' you wonder what was in it before."
What I realized from this paradigm shift was a sad, sad truth... that such concept had to be coined, made and taught -when it is an obvious common sense. Dr. J who thinks ethics taught in medical school is an absolute bogus sometimes expresses too strong of an opinion for me, who is a complete outsider (at least it is hard to identify with his perception at this point in my life). But given that, "policy are often made as are with campaign, by people "not in the trenches", it's rather hard to see the rational behind some of the stuff." So things are kind of out of touch with reality in a sense.
Let's think back what I remember from patient-centered-care.
That everyone is a part of a team, every professional should be well-respected and that they share a common goal - which is to say for patient's best interest - with patient-centered.
But, when you meet some of the patients who demand too much of a health care that shouldn't give them too much privilege (because of their crying and nagging and threats) - ie.// medically irrelevant procedure which patient expects to be billed under the health care - you think if the policy itself may not be so perfect after all.
It sounds good, it looks good, but just not realistic "in the trenches"
Saturday, 19 January 2013

I like being a tourist.
Every little things look more vivid and precious.
You take notice of flickering light in a street and
think how wonderful it is and take note of it.
think how wonderful it is and take note of it.
I mean, When will you come to this place again to take note of it?
Being a tourist anywhere in this world
makes you little more brave,
almost as if your inhibition is loosen,
as if you are drunk,
feeling the buzz.
You become more yourself...
not bound by who [you] are
when [you] are living in a familiar place,
that is... where [you] are from,
where [you] are defined by [you]r work,
[you]r friends and [you]r social circumstance.
You invent yourself but at the same time,
you could be yourself completely.
Since no body has any image of [you].
This is how I mean.
And you can very well tell that
What I don't like are:
Image.
Prejudice.

Perhaps that is why I'm at most ease and friendliest when I don't know people.
Being a tourist allows me to do that.
Being a tourist makes me appreciate things and life in a different light.
Being a tourist also allow me to express the joys with others,
who are also foreigners there.
Being a Tourist


Subscribe to:
Posts (Atom)