Nervous, I showed up 30 minutes earlier than the appointed time.
While waiting, I try to read a book, unsure of things I'm supposed to do.
Quarter past, Dr.T came. He asked if I could run in my shoes. I answered yes.
We run past people, bypassing elevators, using stairs and running through the secret underground passage. During this brief morning exercise, I can feel my brain being picked at and learn about Dr.T's clinical philosophy.
We arrive just in time for the delivery.
In absolute awe, I'm not sure if I introduced myself properly to the parents. I'm not sure how I'm perceived, but I'm there, looking at the whole labor and delivery process with my own eyes, real-time.
The baby almost looks alien as his head peeks out, blue and purple.
umbilical cord cut, baby's first cry is heard, he turns to red and the neonatal unit measures baby's birth weight. Numbers I would often ask parents of the ped patients at Dr.J's office.
Placenta comes out and blood is drawn.
I wonder if any genetic tests are done with those blood?
After the delivery, we go back to the clinic. Everything is electronic and surreal.
The awe of birthing process still not washed away. I noticed sweat marks on back of Dr.T's shirt.
And I take notes on things that I don't understand.
Hereditary spherocytosis
Description:
inherited, clinically heterogeneous red blood cell membrane disorder characterized by spherical erythrocytes, hemolysis, and anemia(1, 2, 3)
I guess I thought about it, but it didn't really dawn on me until I started talking to my mum about the day.
just thinking about it still puts tears in my eyes.
*
Our first patients are people who generously donated their body for education purposes.
Deep inside the university in a newly renovated lab lies ~60 bodies.
Embalmed and ready to go.
Faces, hands and feet were covered because they are all very defining features of 'human'. It brings realism to them.
Before we went to the lab, the instructor said we would get hungry so eat a big meal before the lab and after. Actually smells of formaldehyde and fixing solutions are too strong so it turns off your appetite. You can literally taste the air, of its bitter taste and you know its toxic. Small droplets floating in air are probably fixing tiny portion of proteins in your body.
He was right, you become so hungry.
*
There's a special program where medical students can get a better perception of being a patient with chronic illness. And I will be participating in that program as well.
My partner and I were paired with an adorable sweet boy.
We are still trying to understand what happened to him.
It seemed to me, just a really bad combination of congenital as well as medical error resulted him being the way he is.
His prognosis is an open question.
While talking to the parents, I found out that my partner has MS (Multiple Sclerosis).
Whenever I hear about MS I think about myelin sheath because it is a demylienating condition leading to no sensation and paralysis.
The level of severity may differ but I always think about a woman in a wheel chair at SPU who shared her story with me at 7am in the morning at the University Hospital on a cold night.
*
So young.. my partner is 7 years younger than I am. younger than my little sister.
To know about the pending condition, and still pursuing this very consuming career. I could only show my admiration towards him. Adoration and admiration both.
Wow, so many visits to my small blog.
I was surprised by the number of visits and no comments. I guess my writing still does not elicit any response of readers.
But if you are regular, welcome and I hope my notes are helpful.
*
Some terminologies hemotypsis: hemo- blood + ptysis - act of spitting nulliparous: nullus -not any + para>20 wks births; no pregnancy Gravidity: gravis - heavy; # of times a woman has been pregnant
Some concepts
Gravida (# of pregnancy including current one)/Para (>20 wk births including viable and stillbirths)/Abortus (miscarriage or abortion)
G5P1: pregnant 5X 1 birth
G1P1: That of a woman who has had one pregnancy of twins with successful outcomes
Fetal Non-Stress Test (NST)
- measures heart rate of fetus and its typically higher. Look for deceleration and acceleration. Deceleration means fetal head compression-- good indicator for whether c-section is required or not.
Why ASA and tylenol is ok for pregnant women but not advil? advil (Ibuprofen) has an effect on prostaglandin system. That is why it is not recommended - as with any anti-inflmmatory.
*
Some facts
you can get acute tubular necrosis from prolonged surgery via hypoperfusion due to vasodilating anesthetic
Prolonged nulliparity is a risk factor for breast cancer (think too much hormone!)
no anti-inflammatory/antibiotics for pregnant woman
Right now my room is a mess, so is my kitchen, my inbox, study notes, but most importantly my brain.
I have once told my parents that sometimes my room reflect how my brain is, but I'm not sure if having messiness around me, reflecting my inner state, is helping or not. probably not...ok I will clean.
Anyhow, leaving behind my failure... H** application, G********, C***,
I have received my white coat, soccer jersey and C** member number. Yay!
*
I think writing and organizing my thought helps me to set priorities.
*
One thing about history taking is that doctors need to remember that patients are human.
As well as hard science and medicine, shifting focus to the social and emotion of it would help reveal the diagnosis. At least to narrow down to which diagnosis from the differential.
What I meant to say is that social history is important open-minded question is important
attention on flags!
*
History taking...it goes something like this.
-ID: Patient Id
-CC: current condition
-HPI: history of presenting illness
-Past medical/surgical history
-family history
-allergies
--Physical findings
However, asking if patient is a smoker or drinker is also important.
And social historysuch as their occupation and their relationship is also important. Recent travel history is important and then Paraphrasing!
For me, I switch into screener mode as soon as I have to show my history taking skills to someone else. I don't have any elaborate mechanism but I remember the sheet in the chart and use that as a schema.
One interesting thing learned: Common Depression Screening.
Overwhelming was what I felt as I was introduced to the curriculum. Dr.T going through curriculum and talking about oh-so-many different items. I wasn't hyperventilating, but I felt like I had to.
[Hyperventilating --> means increased PO2 and decreased PCO2. If the blood pH is less than 7.4, metabolic acidosis but since the compensatory mechanism - may be combined with respiratory alkalosis (look at HCO3 level)]
*
So far we have met 2 patient cases. Trauma patient and cancer patient. who knew trauma patient (ie.// stabbing) could have their kidneys affected to the point where it would threaten the life.
*
2 guest speakers. Father of adult down syndrome and breast cancer previvor.
*
We are learning about differential diagnosis. Who knew dry cough could be caused by ACE inhibitor (HBP med) but also from GERD? Who knew DVT could be caused by oral contraceptives?
*
Still struggling with research and being a critical reader to find the best possible resources for patient care.
Whenever I would encounter something, I would write on a scrap piece of paper thinking that it would be good to review and make post out of.
However, this practice was lost in between my procrastination and laziness.
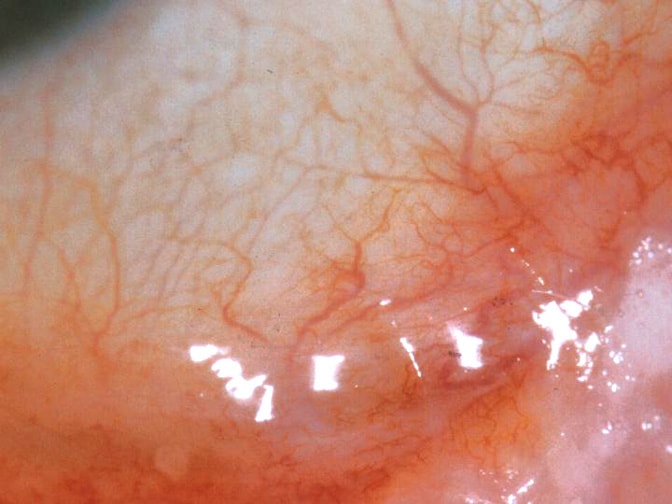
Today as I witnessed tarsorrhaphy (sewing eye lids shut) for the first time, and then I realized I must write about this. After all, my time at the clinic was ending and perhaps this would serve as a good reminder when I have to study ophthalmology.
The patient was a frail woman, octogenarian.
The procedure done was very similar to this, except both medial and lateral corners were done so that there was a 'tiny peep hole' in case something happened to her good eye.
The reason why the mucous membrane is shaved is because cells adhere better.
Sort of like debridement in a way, it just heals better.
The healing was especially important part as the woman had shingles and therefore had lost all her sensation.
"No sensation, No healing"
The reason why tarsorrhaphy is done can be divided to 4 main reasons:
1. Neuroparalytic :Neuroparalytic keratitis is inflammation of the cornea as a sequel to interruption of sensory impulses over the fifth (trigeminal) cranial nerve. The cornea’s loss of sensitivity leaves it much more subject to injury, exposure, and infection.
2. Neurotrophic
3. Corneal disease
4. Decrease exposure.
HERPES ZOSTER --> SHINGLES --> CN 7/ CN 5 damage --> ECTROPION/KERATITIS --> ECTROPION REPAIR/ worst case: TARSORRHAPHY
and as you might have guessed, the woman suffered from shingles and suffered terrible keratitis.
HM (Hand Movement) and LP (Light Perception) was the only vision she had left.
She hardly felt anything was the local anesthetic was given to her (usually "for 7 seconds it hurts like hell!" but "hurts going in but not coming out").
Indeed the surgery was done accordingly and smoothly.
I hope her quick recovery.
*
When CO2 laser is used it can blow 'air' in and can result in subcutaneous emphysema (I google it and it says sometimes referred to Sub Q Air).
Emphysema means 'trapped air'
Usually this can also happen if someone gets DCR (dacrocystorhinostomy) because some bone is removed and so when a person blows his/her nose really hard, it can happen.
*
It is always so difficult to leave the 'position' because you become familiar with it and you identify yourself with the position.
I've had in total about 4 different position here and each leave was 1) Silent (Mutual?) 2)Lots of Yelling P/O 3) Voluntary half fired half? 4) Voluntary
I was given exit review.
1. What did you enjoy the most while working here?
Learning. To be able to witness and participate in all aspect of patient care including reception to screening and assisting was an amazing experience! The sense of fulfillment and really feeling like a part of a team working efficiently together for excellent patient care was another part I enjoyed thoroughly.
2. What did you find the most frustrating?
I don't think I was ever frustrated with anything.
3. Did you feel that management supported you?
Definitely, I was grateful for management's understanding with my volunteer and family commitment.
4. Were you given appropriate training?
Yes, while the course from SAIT provided me with academic guidance on-the-job training and guidance provided by all the other staffs (Olga, Teresa, Cheryl, Angela and Mary) helped me enormously and gave me practical understanding.
5. Were you fairly treated? were your accomplishments acknowledged?
I believe so. Yes, staffs were very appreciative and I was always so flattered.
6. Was your salary reasonable and appropriate
It was discussed.
7. Were your working condition satisfactory?
Sometimes long hours were exhausting (10 hours) but I have no complaints because I enjoyed the OR time
8. What are our office's strengths?
Strong team work, staffs' dedication to excellent patient care, professionalism, efficient staffs, caring environment, friendliness to mention few.
9. What are our office's Weaknesses?
Can't think of any
10. What would you like to see change at the office?
I would not change much, because I considered the office the most ideal in terms of how the clinic should be run. However, I wish sometimes people could be more courteous to one another if they are having a bad day because it is really infectious.
11. Are there any other areas you'd like to discuss?
Thank you very much for everything. I feel so lucky to have worked at this office and feels sorry for leaving, because I can't imagine a better office environment to work.
These days either I'm forgetful or there has not been any new significant 'lessons' for me to post in this blog.
Perhaps, it could be that I have been preoccupied.
*
Dr.J makes a very careful approach in treating his patients.
He is polite but says things that are appropriate in bull's eye manner. I would think it would take me forever to say things in that kind of manner or comes up with the vocabulary that can adequately leaves both the patient and myself perfectly content in communicating the patient's problem. Not exaggerating, but also not undermining - making my observation know if the patient shows discontent know when to move on or 'release the patient'.
The tone, the hand gesture, body language and words he choose seems to be all carefully planned.
I wonder how long and how many times you have to say it that way consciously in order to make it completely yours, which is more automatic, second-nature in a sense. Having the 'right' manner seems to be so difficult.
I have been told I think too much and over-analyze. I do, especially when it concerns what I say or do to people around me. I try to analyze how this person might have perceived me, did I creep that person out? I wonder what our next encounter will be alike? I hope this person doesn't talk about me... along that line almost obsessively. It goes both ways actually. Certain vocabs, words or things that a person says I take it as a hint.
Anyway, back to the lesson. On Thursday - my late night, we had one patient over who used own grocery store in a small town. The grocery store has been in family for 3 generations and he has sold it because such good offer came through. However, due to the effect of giant corporation, a la costco, a la walmart, a la target and etc, the new owners also had 2 other grocery stores but had to close those stores and was struggling with the store this patient sold to them.
Dr.J was more lively when he was talking to the patient during the surgery.
I was thinking that they must have lot of common because Dr.J and patient seemed to find each other pretty engaging when it came to certain topic.
However at the end of the day, Dr.J told me the reason why he kept the conversation going. The patient was on anxiety pill and that the local-anesthetic was not only the mixture of xylocaine and marcaine (6:4) but also the conversation.
I kept thinking I wonder how much Dr.J knows about me, how much he has analyzed me and etc.
Whenever I see this word, I think about media - when socially outrageous, high-profile case takes place in a court house, judge typically "gag order" which bans journalists, juries or anyone associated with the case to not to speak a word of it outside the court.
Would you believe it if there is a similar thing in a contract that your physician signs when they sign with a big hospital ( such as hospital privileges)?
I didn't know about this until today and I also learned that you are not to divulge anything that will harm the hospital's image or which taints the institution, or it's leader's competence or reputation.
You are not allow to criticize for some of the obvious dumb things that executives do and you are not to voice any opinion if something is not working out (ie.// new policy, hospital culture) or mistakes made (non-negligence or honest mistakes due to communication error) or...
The list would be endless because you are simply not allowed to discuss anything.
This seemed counter-intuitive to me, especially because hospital is publicly-funded and thus it should be more transparent than private.
It should be more progressive because it is publicly-funded.
And then, I thought about common sense (who can criticize the system best other than ones who are directly involved with it - on front-line) and I also thought about big-brother, an Orwellian society.
I live in Canada and Canada treasures its 'Charter of Right and Freedom'. It's a fundamental rights and freedom and we as a Canadian have, respect and extend to others.
So, why is it that freedom of speech should be banned when you are a consultant working for the hospital or directly involved with the care for patients, who are Canadians, who pays tax which pays for the service?
If there is inefficiency in the system, it should be voiced and fixed.
If something should be reported, it should be made known to all and fixed.
Why can't we think about fundamentals? Why does the hospital exist in the first place? Who actually does the work at the hospital? Why can we think about the common sense?
There is a really easy-going doctor from South Africa.
He is a practicing physician here and he once said, "South Africa is a 3rd world country with 1st class medical care and Canada is a first class country with 3rd world medical care."
To make things more grim, apparently when you go to a meeting at the teaching hospital, the most discussed subject is Research. That's good... step for innovation and all... and second, which is very, seldom, discussed is teaching....ok....hmmm...skepticism here. Then, what's the third and last thing that is NEVER discussed during these meetings? patient.
I just can't understand the logic...
it seems so blatantly obvious to me that people at that stage should be able to differentiate priorities and discuss about it.
You should save, be efficient and innovate like a private company. There is an absence of any 'push' to get things done in a public system, because after all there's no fiscal year report that sets out the profits or loss, you will forever be paid the salary which increase with every year you are with the government and get pensions and health care. You don't work on holidays, oh wait bank holidays and holidays that are not quite 'red colour' yet. Sounds like a dream job, but at the same time, a leech.
Best of all, the people who are at the management level at the hospital has nothing to do with health or medicine. They have not been fully exposed to front-line work.
They are oblivious about what works and what does not and what leads to inefficiency, and they are controlled by politicians who are then controlled by big companies, who are subsidized by the governments.
This is a loop but for some reason majority of number lose out, sort of like a lottery.
I end my thoughts and discovery I made with this video.
And then just because of the way I am (...) and because I just found this...critique of the above video
... but I realized about half in, he was nit-picky about things that were not so critical and completely missed the point... saying that even if we seize all assets of top 1% it will still not be enough to cover the deficit and so on when Anne was clearly talking about principle, how the subsidy has contributed to the deficit.
Thus, I decided to unpost the critique video because it did not have a nutritious value in my opinion.
Retinoschisis (RS): Disease of the nerve tissue in the eye - affecting retinal cells in the macula
It is a form of a macular degeneration but many people with macular degeneration does not have retinoschisis. Genetic eye disease; male
****- schisis: splitting; breaking up of attachement or adhesion***
Symptoms
Decreased vision (central vision can be affected)
Loss of peripheral vision
Different from retinal detachment.
Retinal detachments can occur if the anchoring of the outer layer of the retina to the eye wall is impaired (bubble inside the wall paper)
Macular degeneration: breakdown or damage to the macula
1) Dry type: Common +++ - tissue becomes thinned and cease to function properly
2) Wet type: damaging +++ caused by the growth of abnormal bv behind the macula. The bv hemorrhage or leak and scar tissue forms if left untreated. Dry type can turn to wet type.
Shingles infection (Herpes zoster) affects CN7 (facial nerve) near your ear. Main symptoms: painful red rash with fluid-filled blisters on, in and around one ear; facial weakness Results in: painful shingles rash, facial paralysis and hearing loss. Treatments: high dose anti-viral treatment and corticosteroids
OCP (Ocular cicatrical pemphigoid)
OCP - stage 2
Subset of the mucous membrane pemphigoid (MMP);
Autoimmune disease characterized by T-lymphocyte dysregulation - the production of circulating autoantibodies directed against a variety of adhesion molecules in the hemidesmosome-epithelial membrane complex --> can affect the skin and other mucous membranes (oral, pharynx, larynx, trachea, esophagus, vagina, urethra, anus); chronic cicatrizing conjunctivities. Characteristic: Slowly progressive and bilateral blinding Average age of onset: 50-60 y.o
Aarskog syndrome
Heritable disease (x-linked), distinctive facial feature Facial feature: such as widely spaced eyes (hypertelorism), a small nose, a long area between the nose and mouth (philtrum), and a widow's peak hairline. They frequently have mild to moderate short stature during childhood, but their growth usually catches up during puberty. Hand abnormalities are common in this syndrome and include Some people with Aarskog-Scott syndrome are born with more serious abnormalities, such as heart defects or a cleft lip with or without an opening in the roof of the mouth (cleft palate)
Hand abnormalities are common in this syndrome and include Short fingers (brachydactyly), curved pinky fingers (fifth finger clinodactyly), webbing of the skin between some fingers (syndactyly), and a single crease across the palm
.
Affects development of many parts of the body.
While it is reassuring to know that Canada ranks within the top 10 in perceived corruption index (which means, it is perceived clean), there are definitely rooms for much improvement.
Note: This shows merely a 'perception' of corruption.
Perhaps people in countries such as Canada are better at hiding their corruption or have legalized it*.
The reason why I'm writing about this issue is because I am passionately against public-sector corruption and waste of tax money as I have seen many cases of inefficient, irresponsible, incompetent government employees wasting away hard-earned income of Canadian (gathered through Canadian income tax paid to both federal and provincial government as well as sales tax - harmonized tax).
Not coming from the privileged class that benefits or have benefited from these corruptions and scandals and being a mere common citizen, I find that it is outrageous when a country like Canada (which I have very high esteem for) show layers of corruption decaying and destroying social safety net slowly but...surely
To summarize, media-friendly and therefore high-profile class action suit lawyer Tony Merchant has been carefully stowing away money offshore- in Cook's island- to evade tax in Canada.
Senator Pana Merchant, left, was named as a beneficiary of a trust set up by her husband, lawyer Tony Merchant.
He was very clever about it - so in order not to get caught, he managed to avoid any paper trail or tried extremely hard to do that. No fax, no e-mail, no phone calls - correspondence through mail only and he would pay the bank fee in cash in mail - no wire-transfer. He and his wife Pana Merchant, current senator, was so careful that Pana Merchant didn't declare herself beneficiary, which she was - and she also did not report any foreign income.
CRA has actually been on his case for years and to evade this, Tony Merchant took this outrageously disgusting plan to action... Isn't making over 120 million from suiting government 'on behalf of natives' not enough that you have to avoid paying tax? are you forgetting that your wife's also getting paid by the government, with tax payers' money in a form of salary of 130K? for doing....what exactly? what does she do exactly?
This came in light as soon as the massive leak of document revealing undisclosed financial records of more than 100,000 people around the world in relation with offshore tax havens - suspected to include hundreds of Canadians.
And delicately tread they must, as CBC's Amanda Lang is the niece of the recent headliner, Tony Merchant, 'the lawyer' in the above mentioned article - meaning the list must be comprised of very high-profile people very closely connected with the politic. And as in Anna Karenina, where Vronsky is begging other high socialite to invite Anna and include her, the lady says: if she broke the law I don't care, but she broke the rule!! - which means that rule of upperclass people must work differently than us commoners. This hypothesis was actually validated by Senator Downe who is seeking answers from Pana Merchant, 'the senator' in above article that
"The government is not taking any action," he asserted. "You go on the CRA website and you'll see all kinds of examples of Canadians from coast to coast to coast charged and convicted with domestic tax evasion. You'll see carpenters in Eastern Canada, doctors in Western Canada. What you will not see is one person charged with overseas tax evasion….
"Domestically, Canadians are treated one way, and people who hide money overseas — very rich Canadians trying to avoid taxes — are treated completely different. It’s grossly unfair." - files from CBC's Curt Petrovich ---Click here for the full article
The reason why I cry foul, is not because of this recent incident - politician, public sector employees and corruption has always been a synonym. Hardly anything new.
For example, Merali's sinister orchestration with e-health in Ontario which costed previous early retirement of then health minister and millions and millions to tax payer in Ontario, and then our incompetent government not taking any action - despite the fact that it was all OVER the MEDIA!!! but of course in another province, the same corrupt people welcomes him and then gives him all-expense paid by the tax-payer card and he racks up huge expense- big cost to the government. There's an old idiom from sage, "Bitch's habit does not leave the Bitch" and yes, Merali is a living example to that idiom.
All the while, CRA (Canadian Revenue Agency) is understaffed with recent cut introduced by the finance minister Tom Flaherty, and what's more, the CRA has a disgusting habit in that they go after the small fish that does not have political power or the wealth to defend themselves.
They would go for cases that are easy win - independent business owners, doctors and etc - not that they should let them get away - but if someone's evading tax by millions and millions and not thousands, shouldn't you go after those millions and not the thousands?
* Referring to the inefficient and horrible life-time appointment of the senate system (changes made to limit the age of participation/retirement as there were senators who had Alzheimer's who still took part of the discussion making it a laughing stock, as well as sexual assault convict and senate who could possibly be dyslexic as he 'made mistake' from ticking the box asking for yes/no answer (Mike Duffy) and etc)
* Also referring to Toronto Transit Commission ticket collector who makes over 100K, although this is bad management than 'corruption' - but people let it slide were being very noncontinuous with the tax money, thus mismanaging public purse would also mean corruption.
CN3, Oculomotor Nerve, Muscles in Eyes (rectus muscles, oblique muscles), Medication used in Grave's, tapazole, b-blocker, SNS, muller's muscle, Recession surgery, Difference between Horner's and Myasthenia Gravis
In my scrap sheet consisting of things that I-must-record-before-I-forget were above words.
What Dr.J went through with me during the surgery day on March 20th.
I remember from with my shameful response that I couldn't answer all the muscles in eyes innervated by which muscles (oculomotor muscle the obvious choice, but there are 2 other nerves that actually affect the eye movement, rather innervates muscles to the eyes moving it up, down, to sides and etc.)
Dr.J said in a teacher's tone, "Use the process of elimination.
Everything is innervated by oculomotor nerve (CN 3) except lateral
rectus muscle which abducts and thus innervated by abducens nerve (CN 6) and
superior by trochelear (CN 4)." Actually I was able to say oculomotor after muttering to myself: ""Oh, oh, oh, to touch and feel very good velvet...ah, heaven."
That was very embarrassing and I didn't have a chance to redeem myself by compensating with the cool knowledge that I had - last time I mentioned SJS (I looked it up!) after blundering the basic concept to compensate my stupidity (to save thy face!).
The talk of extraocular muscle came after asking Dr.J about the recession surgery done on thyroid patients who has proptosis or exopthalmos. Typically with age, you have dermatochalasis and the two approach can be used to solve this problem. Blepharoplasty or ALR (anterior levator resection) surgery
See ALR surgery video here:
While the bleph surgery removes the fat and skin, ALR is the surgery for the muscle directly.
That is why patient have to practice "sit-ups" during the surgery to get the palpebral aperture right (so both eyes are symmetrical).
However, there's the exact opposite surgery which is called the recession surgery which reats the eyelid retraction - where the eyelids are abnormally wide (THYROID!).
Eyelid retraction recession weakens the muscle in the upper eye lid bring the eye lids down.
Anyway, for thyroid patients typically those with Grave's, their thyroid levels is up.
Thyroid level up -->
adrenergic up (that's why their heart beats very fast) -->
SNS activation (travel via carotid artery) -- Postganglionic sympathetic fibers originate in the superior cervical ganglion, and travel via the internal carotid plexus -->
muller's muscle activation (or superior tarsal muscle which is a smooth muscle adjoining the levator palpebrae superioris muscle that helps to raise the eye lid)-->
Proptosis!!
Tapazole and beta blockers are used to treat the grave's
and I have wrote alpha blockers too... interesting that Flomax which is a drug used to improve urination in men with benign prostatic hyperplasia.... is an alpha-blocker thus also treats high blood pressure. I have to review medication yet again...used by patients and used during the surgery... Moving on from Thyroid now, I would like to talk about Horner's and myasthenia gravis. I don't know why but it is very difficult for me to differentiate between the two and I have also confessed this difficulty to Dr.J. Both are manifested by ptosis. With Horner's there's miosis (pupil smaller) and anhydrosis (no sweating) With MG, acetycholine test and ice test. I should know Horner's syndrome as my dad was suspected of having this due to possible tumors Anyway, from Wikipedia:
Horner syndrome is due to a deficiency of sympathetic activity. The site of lesion to the sympathetic outflow is on the ipsilateral side of the symptoms. The following are examples of conditions that cause the clinical appearance of Horner's syndrome:
A patient comes in for consultation and possible (surgery) for ectropion repair.
Something like this.
Right side forehead smooth, eye pulled down - full of tears.
Keratinized and angry looking conjunctiva, man complained of 'hard of hearing' and loss of light perception and sensation from his right eye.
The man smelled certain way and I noticed the old stained overall holding his pants.
After he was seen, instead of ectropion repair, Medial Canthal Tendon repair was to be go ahead with it.
I've never seen the procedure and normally this would be done under Major OR (anesthetic)- but since this man had lost all sensation in his right face - including in his cornea - it was ok.
During the surgery - Dr.Johnson says,
"the one thing that I learned after medical school was that corneal cell regenerates as there are stem cells in limbus - so this man- not being able to feel anything indicates that this is not a normal bell's palsy - It's not just the CN 7 that's affected."
and then he asks me:
"which CN is the one for corneal sensation?"
of course I go, "um..."
"CN 5, trigeminal nerve" this was new to me. I think back from my book if I had ever read something about this. Nope, I didn't see it (later that night I went back to my text book and of course it doesn't say anything... through google I just confirmed this - as I almost wrote CN3 - oculomotor nerve)
And then the man says, "my hearing is bad in one ear (indicating his right where the bell's palsy was)"
Dr.J exchange looks with me and says, "and also the CN 8 - there's something going on."
I noticed that near his jaw and neck, there's a overly protruding bone (?) and I point at that as I wonder.
Dr.J nods then says "five."
No light perception..I wonder if his right pupil constricted? because this would indicate that his CN3 was also affected.
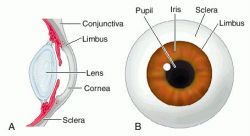
Back to limbal epithelial cells of the cornea.
During undergrad, I had the most difficulty wrapping around the concept of stem cells and to this day, I'm quite confident to say I don't understand whole lot what's going on with the cell development.
I know that there are different levels of stem cells such as totipotent (total: can make an individual!!) and pluripotent (sublevel: not fixed as to developmental potentialities; especially: capable of differentiating into one of many cell types) cells and then it gets complicated....
Summary for myself (short copy and paste from the above link):
Ok, so what is cornea?
The cornea is responsible for protecting the eye against insults such as
injury and infection. It also provides the majority (two thirds) of the
total refractive power of the eye and is therefore the major refracting
lens (Meek et al., 2003). So the LASIK, LASEK surgery is basically carving the corneal to correct the refractive power.
The corneal epithelium is a dynamic physical barrier preventing the
entry of deleterious agents into the intraocular space. It consists of
superficial squamous cells, central suprabasal cells and a single layer
of inner columnar basal cells (Seckera& Daniels 2009).
Corneal integrity and therefore function is dependent upon the
self-renewing properties of the corneal epithelium. The prevailing
hypothesis is that this renewal relies on a small population of putative
stem cells located in the basal region of the limbus (Seckera& Daniels 2009).
that's what Dr.J said!!!
Throughout life, our self-renewing tissues rely upon populations of stem
cells / progenitors to replenish themselves throughout life following
normal wear and tear and injury. The corneal epithelium on the front
surface of the eye is no exception as dead squamous cells are constantly
sloughed from the corneal epithelium during blinking. At the
corneo-scleral junction in an area known as the limbus, there is a
population of limbal epithelial stem cells (LESCs). LESCs share common
features with other adult somatic stem cells including small size
(Romano et al., 2003) and high nuclear to cytoplasmic ratio (Barrandon and Green, 1987). They also lack expression of differentiation markers such as cytokeratins 3 and 12 (Kurpakus et al., 1990; Schermer et al., 1986).
The Canadian Press / Handout / University of Alberta-Michael Holly"What means the most to me is what our work means to patients. Some people think this may hurt my chances for the Nobel, but I felt that this is the time to stick my feet in," Michael Houghton told the Post
It’s a respected medical research award, dubbed the “baby Nobels” as many of its winners have gone on to earn the coveted science prize. But Edmonton’s Dr. Michael Houghton has declined the Canada Gairdner International Award, worth $100,000, for his contribution to the discovery of the hepatitis C virus. He said he couldn’t accept the honour, also awarded to Dr. Harvey Alter of the National Institutes of Health, Dr. Daniel Bradley of the U.S. Centers for Disease Control and Prevention, if two other important researchers on his team were shut out. The Canada Excellence Research Chair in Virology said awards committees are stuck in the past, unwilling to acknowledge that research teams have grown since the time of Alfred Nobel. He spoke with the Post’s Sarah Boesveld from his office at the University of Alberta.
Q: Explain a bit further why you’re not taking the award.
A: I believe there were five key contributors: The three that received the Gairdner Award [which includes Dr. Houghton,] and Dr. George Quo and Dr. Qui-Lim Choo [who are employed by Chiron Corp.) Those two people worked with me for seven years to discover the virus in my laboratory.
Q: Do you think they were shut out because they work for a private company?
A: Oh, I don’t know. First of all let me say I’m pleased for Dr. Alter and pleased for Dr. Bradley — those two individuals made important contributions. I just feel that this is yet another example — and this is not the first time — of where a major discovery is done by a number of people, but when it comes to recognizing that discovery, they’re exclusive rather than inclusive. The facts are, these big discoveries these days need big teams.
I haven’t told my wife that yet.
Q: Why are the awards so exclusive? The pot of money?
A: No, I don’t think it’s that. It’s all based on the Nobel prize. In his will, Dr. Nobel says there can be no more than three. All of the other major awards tend to copy that and limit it to three. It’s antiquated. In the days of Nobel, research was done by one or two people in small labs. Now it’s done by big teams in multiple labs. I’m very grateful to the Gairdner, I highly respect them, they do a fantastic job. On this one, unfortunately, I couldn’t accept.
Q: Why take such a stand when you could have accepted and acknowledged their major contributions?
A: I think I’ve evolved my philosophy after many, many years. When you make a big discovery, nobody trains you on how to handle it. In the 1990s, I got a call from the Robert Koch Foundation offering an award to myself and Dr. Bradley. I requested Dr. Choo and Dr. Quo be included and they said no. I took the award anyway. In the 2000s, I got a call from the Lasker Committee who said I got the award with Dr. Alter. I said ‘It’s really important that Dr. Quo and Dr. Choo be included.’ They said no. I agonized over the Lasker for many weeks and eventually I decided to accept it.
What means the most to me is what our work means to patients. Some people think this may hurt my chances for the Nobel, but I felt that this is the time to stick my feet in
Q: How do Drs. Quo and Choo feel about it all?
A: They feel they deserve direct recognition and I agree with them. I think it was after the Lasker that I decided ‘well, I really shouldn’t do this anymore.’ I never envisaged a situation when I was offered an award, I couldn’t persuade the committees to include my colleagues. That’s been a complete shock to me. It’s a huge disappointment. It takes a lot of the pleasure out of the whole process. It makes it awkward. It makes it unpleasant.
Q: Do you think this will hurt your chances at getting a Nobel prize?
A: I’m very respectful of the Nobel and the Gairdner and the Lasker and Robert Koch. What means the most to me is what our work means to patients. Some people think this may hurt my chances for the Nobel, but I felt that this is the time to stick my feet in. This was the opportunity to do it.
My thoughts: it is so rare to see works credited to post docs and fellows who actually does bulk of the work in research. And when I say the bulk of the work, I mean: proposals, actual research - procuring specimen, experiment, statistic analysis, writing. Of course supervisors are some-what involved...actually the level of involvement between P.I (Primary Investigator) differs quite a lot that you can not generalize.
Knowing this, reading the article struck me with a thought.